
According to a research report by the World Health Organization, the number of myopia patients in China reached as many as 600 million in 2018, and the myopia rate among teenagers ranked first in the world. China has become the world's largest country with myopia. According to the 2021 census data, the myopia rate accounts for about half of the country's population. With such a large number of myopia people, it is very important to scientifically popularize myopia-related professional knowledge.
The mechanism of myopia
The exact pathogenesis of myopia is still unclear so far. To put it simply, we don’t know why myopia occurs.
Factors associated with myopia
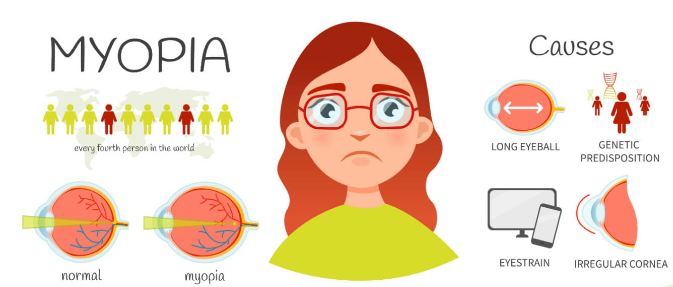
According to medical and optometry research, the occurrence of myopia is affected by many factors such as genetics and environment, and may be related to the following factors.
1. Myopia has a certain genetic tendency. As the research on the genetic factors of myopia becomes more and more in-depth, especially pathological myopia has a family history, it is currently confirmed that pathological myopia is a single-gene genetic disease, and the most common is autosomal recessive inheritance. . Simple myopia is currently inherited from multiple factors, with acquired factors playing a major role.
2. In terms of environmental factors, factors such as long-term close reading, insufficient lighting, too long reading time, unclear or too small handwriting, poor sitting posture, malnutrition, reduction in outdoor activities, and increased education level may be related to the development of myopia. occurrence related.
Classification differences of myopia
There are many classifications of myopia, because the cause of onset, the cause of refractive abnormalities, the degree of myopia, the duration of myopia, stability, and whether adjustment is involved can all be used as classification criteria.
1. According to the degree of myopia:
Low myopia: less than 300 degrees (≤-3.00 D).
Moderate myopia: 300 degrees to 600 degrees (-3.00 D~-6.00 D).
Myopia: greater than 600 degrees (>-6.00 D) (also called pathological myopia)
2. According to the refractive structure (direct cause):
(1) Refractive myopia, which is myopia caused by an increase in the refractive power of the eyeball due to abnormal eyeball refractive components or an abnormal combination of components while the axial length of the eye is normal. This type of myopia can be temporary or permanent.
Refractive myopia can be divided into curvature myopia and refractive index myopia. The former is mainly caused by excessive curvature of the cornea or lens, such as patients with keratoconus, spherical lens or small lens; the latter is caused by excessive refractive index of aqueous humor and lens, such as primary cataract, iris-ciliary body inflammation patients.
(2) Axial myopia: It is further divided into non-plastic axial myopia and plastic axial myopia. Non-plastic axial myopia means that the refractive power of the eye is normal, but the length of the anterior and posterior axis of the eyeball exceeds the normal range. Each 1mm increase in the eyeball axis is equivalent to an increase of 300 degrees of myopia. Generally, the diopter of axial myopia is less than 600 degrees of myopia. After the diopter of partial axial myopia increases to 600 degrees, the axial length of the eye continues to increase. The myopia diopter can reach more than 1000 degrees, and in some cases even reaches 2000 degrees. This kind of myopia is called progressive high myopia or deformed myopia.
The eyes have various pathological changes such as high myopia, and the vision cannot be corrected satisfactorily. This type of myopia has a family history and is genetically related. There is still hope for control and recovery in childhood, but not as an adult.
Plastic axial myopia is also called plastic true myopia. Reasons, such as lack of vitamins and trace elements during the growth and development period can cause myopia, as well as myopia caused by ophthalmia or physical diseases. It is further divided into plastic temporary pseudomyopia, plastic intermediate myopia and plastic axial myopia.
(a) Plastic temporary pseudomyopia: This type of myopia takes a shorter time to form than plastic temporary pseudomyopia. This type of myopia, like accommodative temporary pseudomyopia, can return to normal vision in a short period of time. Different types of myopia require different recovery methods. Characteristics of plastic temporary pseudomyopia: when factors are corrected, vision improves; when new factors arise, myopia continues to deepen. Generally, there is a plasticity range ranging from 25 to 300 degrees.
(b) Plastic intermediate myopia: The visual acuity does not improve after correcting the factors, and there is no plastic true myopia that extends the visual axis.
(c) Plastic axial myopia: When the plastic pseudomyopia in the axial myopia type develops into plastic true myopia, it is more difficult to restore vision. Myopia recovery training 1+1 service is used, and the recovery speed is relatively slow. It requires The time is also very long.
(3) Compound myopia: the first two types of myopia coexist
3. Classification according to disease progression and pathological changes
(1) Simple myopia: Also known as juvenile myopia, it is a common type of myopia. The genetic factors are not yet clear. It is mainly related to the high-intensity visual load during adolescence and development. With age and physical development, at a certain age, will tend to be stable. The degree of myopia is generally low or moderate, the myopia progresses slowly, and the corrected vision is good.
(3) Pathological myopia: Also known as progressive myopia, it mostly has genetic factors. Myopia continues to deepen, progresses rapidly during adolescence, and the eyeball is still developing even after the age of 20. Visual function is significantly impaired, manifested by lower than normal distance and near vision, and abnormal visual field and contrast sensitivity. Accompanied by complications such as retinal degeneration in the posterior pole of the eye, myopic arc spots, macular hemorrhage, and posterior scleral staphyloma, the disease progressively deepens and develops; the vision correction effect is poor in the late stages.

4.Classification according to whether there is any adjustment force involved.
(1) Pseudomyopia: Also known as accommodative myopia, it is caused by long-term close work, increased visual load, inability to relax, accommodative tension or accommodative spasm. Myopia can disappear through medication to dilate the pupils. However, it is generally believed that this type of myopia is the initial stage of myopia occurrence and development.
(2) True myopia: After using cycloplegic agents and other drugs, the myopia degree does not decrease or the degree of myopia decreases by less than 0.50D.
(3) Mixed myopia: refers to the diopter of myopia that has been reduced after using cycloplegic drugs and other treatments, but the emmetropic state has not yet been restored.
True or false myopia is defined based on whether adjustment is involved. The eyes can zoom by themselves from far to near objects, and this zooming ability relies on the adjustment function of the eyes. Abnormal accommodation function of the eyes is further divided into: accommodative temporary pseudomyopia and accommodative true myopia.
Accommodative temporary pseudomyopia, the vision improves after mydriasis, and the vision improves after the eyes rest for a period of time. In accommodative intermediate myopia, the visual acuity after dilation cannot reach 5.0, the eye axis is normal, and the periphery of the eyeball is not extended anatomically. Only by increasing the myopia degree appropriately can the visual acuity of 5.0 be achieved.
Accommodative true myopia. It refers to the failure of accommodative pseudomyopia to be recovered in time. This situation lasts for a long time, and the eye axis is lengthened in order to adapt to this near vision environment.
After the axial length of the eye is lengthened, the ciliary muscles of the eye are relaxed and the convexity of the lens returns to normal. Myopia has completed a new evolutionary process. Each axial length of the eye is extended by 1mm. Myopia deepens by 300 degrees. Accommodative true myopia is formed. This type of true myopia is essentially different from axial true myopia. This type of true myopia also has the possibility of vision recovery.
Supplement to myopia classification
We need to know here that pseudomyopia is not medical "myopia" because this "myopia" can exist in anyone, in any refractive state, and at any time, and the eyes will be tired. The myopia that disappears after the pupils are dilated is pseudomyopia, and the myopia that still exists is true myopia.
Axial myopia is classified based on the cause of abnormalities in the refractive media within the eye.
If the eye is emmetropic, the various refractive media in the eye just refract the light onto the retina. For people who are emmetropic, the total refractive power of the various refractive media in the eye and the distance (eye axis) from the cornea at the front of the eye to the retina at the back are exactly matched.
If the total refractive power is too large or the distance is too long, the light will fall in front of the retina when looking far away, which is myopia. Myopia caused by high refractive power is refractive myopia (caused by corneal abnormalities, lens abnormalities, cataracts, diabetes, etc.), and axial myopia caused by the elongation of the axial length of the eyeball beyond the emmetropic state (the type of myopia that most people have) ).
Most people develop myopia at different times. Some are born with myopia, some are myopic in adolescence, and some become myopic in adulthood. According to the time of myopia, it can be divided into congenital myopia (myopia is born), early-onset myopia (under 14 years old), late-onset myopia (16 to 18 years old), and late-onset myopia (after adulthood).
There is also whether the diopter will change after myopia develops. If the diopter does not change for more than two years, it is stable. If the diopter remains long within two years, it is progressive.
Summary of myopia classification
In the fields of medical ophthalmology and optometry, there are many other classifications of myopia, which we will not introduce due to microscopic expertise. There are so many classifications of myopia, which are not conflicting. They just reflect the complexity and uncertainty of the mechanism of myopia occurrence and development. We need to describe and distinguish categories of myopia from different aspects.
The myopia problem of each of our myopic people must be a branch of the corresponding myopia category. It is undoubtedly unscientific to talk about myopia prevention and control regardless of myopia classification.
Post time: Nov-24-2023